95 Scripps Dr, Sacramento, CA 95825
(916) 929-1833

Women consider breast augmentation for various reasons. Sometimes it’s because they were dealt a raw deal from the get-go, or sometimes after pregnancy they wonder what happened to their nice-sized breasts. As long as the breast skin envelope is still in good shape, and the nipple/areola hasn’t dropped too low, then adding a breast implant can be a perfect solution. The implant can fill up a loose skin envelope (after pregnancy and breast-feeding) making the breasts look full again. For small-breasted women, adding an implant can enlarge the breast so that it is more proportional and pleasing.
Breast implants can be either saline-filled or silicone-filled. Both types of implants come in a variety of sizes, as well as varying projections. The most important tool I use to decide which implant size to use are the woman’s actual breast dimensions. The implant should “fit” a woman’s breast, having the same cleavage curve, so as to look the most natural. When you see women who don’t look natural, it’s because they have implants which don’t fit their breasts. A “too big” implant tends to look too high, with a sharp forward projection, or it sticks out the side of the chest too far. A “too big” implant also tends to deform the breast over time, stretching the lower breast skin (“bottoming out”) which can result in nipples pointing at the ceiling. During your consultation, I will take some measurements of your breasts, and let you know the range of sizes that will “fit” your body. Hopefully, an implant in that range will achieve the look you are seeking.
In deciding between silicone and saline, a woman must think about feel, cost, and safety. Saline implants are less expensive than silicone. A higher cost does not mean silicone implants are better, it only means the manufacturers had to spend more money bringing them to market, and are recouping that expense by passing it off to the patient. Saline implants are more “feel-able”. If you had a saline implant in one breast and a silicone in the other, you might not be able to tell there was an implant on the silicone side. However, you would likely be able to tell there was an implant on the saline side because the implant can feel a bit stiffer and you can sometimes feel the implant shell a bit under the surface. The more native breast tissue you have, the less you feel the saline implant. Women who have B-cup or larger breasts can usually pick either silicone or saline, depending on their personal choice. Women with A-cup breasts will likely be happier with a silicone implant, since they don’t have as much “camouflage” to hide the feel of the saline implant.
All implants have a risk of failure. Implants are under-filled, if you will, so that they will feel nice and soft. However, normal life activities can bend and fold the implant a bit. This folding, over time, can result in a crack in the implant shell. If a crack develops in a saline implant, the saline will leak out and the implant will deflate. The good news is that all implants come with a warranty: the manufacturer will give you a replacement implant at no charge at any time (lifetime warranty). If an implant fails within 10 years of your initial surgery, the manufacturer will also help defray the cost of replacing the implant. After ten years, the implant warranty is still good, and the patient can receive a free replacement implant, but she must also bear the cost of the operating room, etc. on her own. Saline implants fail in about one out of every five patients. Implants don’t need to be replaced unless they fail. Breast implants are not like tires you have to rotate! Four out of five women will not have a failure at all.
With silicone implants, there is also a risk of failure. However, when a silicone implant fails it may not be noticed because the shape and size of the breast remain the same. This is a “silent” failure, because the silicone is “cohesive”. It sticks together and is not absorbed by the body. Silicone implants need to be monitored over time. My rule of thumb is to start imaging the implants with either ultrasound or MRI starting about five years after augmentation to check the integrity of the implants. If the implants look fine, then they are rechecked every couple of years. If a failure is detected, then the warranty applies and a new implant will be provided. Silicone failures, however, can require additional removal of the body’s naturally-created scar capsule that surrounds the implant, to assure complete removal of all silicone. That can make the replacement surgery somewhat more expensive (more OR time) and the recuperation a little slower than with saline-implant replacement.
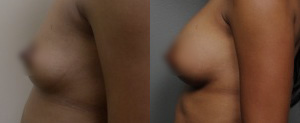
See Before and After Photos of Real Breast Augmentation Patient Results
Breast augmentation can be performed either using general anesthesia or with what is called conscious sedation. Most of my breast implant surgeries are done with this conscious sedation and local anesthesia. Patients are snoozing and very comfortable during the procedure. The surgery takes about two hours, but you arrive an hour before and stay for about two hours after in the recovery room. You go home wearing a soft bra, with some bandages over the incisions.
I want you to be up and moving as quickly as possible, doing some gentle stretching of the chest muscles. The more you move, the better you’ll feel. There are 3-5 days of muscle soreness, sort of like if you did push-ups. The implants tend to look too high and too flat initially. It takes a few days for them to settle into position. Usually you can wear a tank top within 1-14 days. Usually it takes a month or two for the breasts to feel as soft and supple as they will.
Most women take one week off work. Women with more physically demanding jobs may need a little bit more time off. I ask you not to do anything that makes your heart pound, or makes your sweat, for two weeks. This is to minimize the risk of post-operative bleeding or muscle damage. After two weeks you can work back into your normal exercise activities, using how you feel as a guide.
We ask you to return to the office for check-ups 3-4 times in the first month, then usually at 2 months, 6 months, and a year after surgery. It is important to have a breast exam by a doctor comfortable feeling breasts with implants at least once a year. For this reason, I ask my patients to return annually for a no-cost breast exam. In this way, I can check the breast tissue itself as well as evaluate the implants. If you choose silicone implants, then I can also arrange for implant imaging (once you’re about 5 years out), to make sure your implants are doing well.
In a perfect world, you would wait until after you had finished child-bearing before undergoing breast augmentation. We all know that pregnancy and breast feeding can change the size and shape of the breasts. Most women can successfully breast feed after augmentation. The implant is separated from the breast tissue by the pectoral muscle, so it has no effect on breast milk. Once you finish breast feeding completely, you may notice a change in the appearance of the breasts. I always warn women who have not yet had children, or those who might have another child after augmentation, that they might require some “maintenance work” on the breasts, if they don’t like what they see after finishing their child-bearing.
Currently, breast imaging with mammography involves placing the breast between two glass plates and flattening it so as to take a radiographic image of the breast tissue. This involves two pictures of each breast. It is a bit uncomfortable, but not difficult. When you have implants, you must be sure to inform the imaging center of that fact. They will usually make you sign a release that basically says, “If we break your implants it’s not our fault.” I have yet to see an implant that was broken in a mammogram. It’s more important to make sure you don’t have a breast cancer!
Anyway, when you have implants they will take four pictures of your breast: a standard 2-picture squish, and then a second 2-picture mammogram where they try to move the implant out of the way and just image the breast tissue. This is because the implant makes it hard to see some of the breast tissue. By taking additional pictures, the radiologist can adequately monitor your breast health. The extra radiation is negligible, and so it is not dangerous.
The whole point of self-exam is not to try and find “lumps”, but to get to know your breasts well enough that if something changes you will notice it and get checked out. After breast augmentation, it will take you a little bit of time to get familiar with your breasts again, as they will feel a little bit different. All of the breast tissue will be above the implants, so no breast tissue will be “hidden”. If you ever feel anything new and concerning, you should have it checked out immediately. I ask my breast implant patients to re-learn their self-exam after augmentation, and then if they ever notice a change, to come see me right away. Sometimes the change can be due to feeling the implant itself, and that can be quickly determined and your fears allayed. If there actually is something in the breast tissue that is of concern on my exam, I can usually figure out the cause more quickly and cosmetically (with less risk of damaging the implant) than your primary care doctor. Remember, any post-operative visits to check your implants, no matter how long ago they were placed, are free of charge.
Implants do have a risk of failure, but if they aren’t broken there is really not reason to replace them. If a saline implant breaks, you know it right away because of the deflation. You call the office and we will set you up for replacement as quickly as possible. With silicone, you do need to follow-up with imaging of the implants to check for “silent” failure. But, again, there is no need to replace them unless they break. And the odds are in your favor that you’ll never have to replace them.
There is also the risk of what is called “capsular contracture”. This is a firming up of the breast implant caused by the shrinkage of the scar your body naturally forms around the breast implant. Although the risk of capsular contracture is relatively low, it is impossible to predict which woman might be at risk. If you develop scar tightening, you should return to see me immediately, as there are some easy things we can do (medication, laser treatment) that can sometimes nip it in the bud. If the contracture is bad enough, sometimes surgery is necessary to remove the tight scar. The implant might be replaced as well. One of the implant manufacturers (Sientra) will provide a new replacement implant for free for any woman who has to undergo contracture treatment surgery within two years of her original augmentation surgery.
I try to work closely with each woman to decide together about sizing before surgery. There are women who choose the largest implant I think will fit them. If that woman later on feels her breasts are not big enough, I apologize, but tell her that any bigger implant would either look stupid and/or would deform her breast over time. Younger women tend to want larger implants. They sometimes regret this choice as they age, perhaps put on a little weight, and end up with breasts that are too large. I do sometimes downsize implants, but down-sizing might also require a breast-lift (and thus more scarring) so that the breast skin doesn’t look too saggy. I try very hard to counsel patients on implant sizing and what will give them the most natural and long-lasting result.